
A Historic Drop
A new paper details a statewide initiative by the California Maternal Quality Care Collaborative that significantly reduced cesarean deliveries for low-risk babies
It was an alarming trend with seemingly no end in sight. Across the nation, cesarean delivery rates had been increasing for a decade, rising 50% from 2005 to 2015.
Concerned about the safety of these procedures for mothers and babies, the Stanford University–based California Maternal Quality Care Collaborative (CMQCC) decided to take action to reverse the trend. In 2016, the CMQCC partnered with the California Health Care Foundation (CHCF) to mount a statewide hospital quality improvement initiative to reduce the cesarean delivery rate for nulliparous, term, singleton, vertex (NTSV) births — essentially, babies you’d expect to be born vaginally without incident.
Clinical Professor Elliott Main, MD, CMQCC’s medical director, notes that other groups had attempted to reduce C-section rates in the past and failed. “The powers of the status quo were very strong,” says Main.
But the CMQCC hit upon a unique recipe for success. Main is among the co-authors of a paper published in the Journal of the American Medical Association that reveals how a multipronged effort decreased California’s NTSV cesarean rate from 26% in 2014 to 22.8% in 2019 — well below the national target of 23.9%.
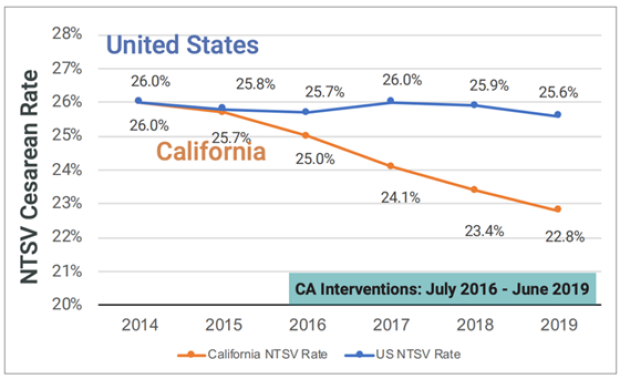
California’s NTSV cesarean rate decreased from 26% in 2014 to 22.8% in 2019.
The key ingredient was collaboration aimed at both the internal (hospital level) and external (statewide) environment. “You needed a lot of people everywhere to get involved to make a change at this scale,” says Main.
Changing the culture
C-section rates in the US vary widely from hospital to hospital — from as low as 7% to as high as 70% —and from physician to physician. Differences in patient populations don’t explain away the variation, suggesting a need to impact hospital unit culture and individual clinician attitudes.
Christa Sakowski, MSN, a clinical lead at the CMQCC and a co-author of the study, notes that a prevailing attitude among many providers has been, “Safe mom, safe baby. Doesn’t matter how the baby comes out,” she says. The belief that C-sections are equivocal to vaginal births has contributed to the high prevalence of these procedures — at the expense of mothers’ and babies’ safety.
While C-sections can be lifesaving procedures, they can also introduce fatal complications for mothers, such as hemorrhage and blood clots. Women who’ve had first-birth C-sections are over 90% more likely to have C-sections for subsequent births, putting them at greater risk of hysterectomy and uterine rupture. And babies delivered by cesarean have a higher likelihood of infection and respiratory complications.
To educate providers on these risks and encourage a cultural shift to favor vaginal births, the CMQCC invited California hospitals with baseline NTSV cesarean rates greater than 23.9% to join one of three cohorts for an 18-month quality improvement collaborative between July 2016 and June 2019. Those that participated met monthly with mentorship groups that included Sakowski and mentor physicians and nurses who shared successful reduction strategies from other hospitals and cohorts.
Nearly all of the hospitals implemented provider education on national guidelines for labor management and increased labor support activities. The majority also availed themselves of rapid-cycle data offered by the CMQCC to internally share physician-level C-section rates. This allowed departments to reward physicians with low C-section rates and address outliers, creating a culture that was more supportive of vaginal births.
“The recentering that C-sections are not equivocal to vaginal deliveries is critically important,” says Sakowski.
A steady drumbeat
Externally, the CMQCC pursued partnerships with nonprofit and governmental organizations. Health plans and purchasers offered incentives for hospitals to participate in the collaborative, while the California Secretary of Health and Human Services gave awards for those that met the national target rate.
The recentering that C-sections are not equivocal to vaginal deliveries is critically important.
Other partnerships helped equip patients with information about C-sections to guide their decision-making. The CMQCC and CHCF collaborated with Yelp to publish hospitals’ C-section rates on their Yelp pages. They also partnered with Consumer Reports to create short animated videos to encourage women to talk to their doctors about how to avoid a C-section.
The repetition of the cesarean-reduction message was by design. “It was kind of a drumbeat,” says Main. “You hear it on this side, you hear it on that side, you hear it up there, you hear it below — and that made a difference.”
A resounding success
The collective effort lowered California’s overall C-section rate and narrowed the variation among hospitals, without any risks to mothers or babies. In fact, severe unexpected newborn complications decreased at participating hospitals.
Both Main and Sakowski are heartened by the results. “It shows that wide-scale improvement can work,” says Sakowski, adding that the CMQCC is actively involved in helping other states mount similar campaigns. “It’s absolutely possible to replicate [the results] with the right resources.”
Rachel B. Levin is a Los Angeles–based freelance writer and editor.

Stanford Ob/Gyn Magazine: Winter 2023
This edition of the annual department publication features the providers building infrastructure out for pediatric and adolescent gynecology, an inside look at community engagement for LGBTQ+ populations, and an astounding improvement in the cesarean section rate made through CMQCC's quality improvement efforts. Read more.